

GUÍA PRÁCTICA CLÍNICA:
PARA EL DIAGNÓSTICO Y TRATAMIENTO DE LUMBALGIA (2016)
DESCARGAR
VERSIÓN ARTÍCULO
DESCARGAR
VERSIÓN EXTENSA
DESCARGAR
ANEXOS
DESCARGAR
VERSIÓN CORTA
DESCARGAR RECOMENDACIONES Y FLUJOGRAMAS
vacio
vacio
Ámbito
- Esta guía debe ser usada en todos los establecimientos del seguro social del Perú (EsSalud), según lo correspondiente a su nivel de atención.
Población y alcance
- Población: pacientes con lumbalgia.
- Alcance: diagnóstico y tratamiento de lumbalgia.
Autores
Expertos clínicos:
- Ricardo Carpio Guzmán
Hospital Nacional Edgardo Rebagliati Martins, EsSalud - José Chávez Corrales
Hospital Nacional Edgardo Rebagliati Martins, EsSalud - Nives Santayana Calizaya
Hospital Nacional Edgardo Rebagliati Martins, EsSalud - Jaime Collins Camones
Hospital Nacional Guillermo Almenara Irigoyen, EsSalud - Jesús Robles Recalde
Hospital Nacional Guillermo Almenara Irigoyen, EsSalud
Metodólogos:
- Adrián V. Hernández
Consultor Metodológico, IETSI, EsSalud - Alejandro Piscoya Rivera
Consultor Metodológico, IETSI, EsSalud
Coordinador:
- Víctor Suárez Moreno
IETSI, EsSalud - Raúl Timaná Ruiz
IETSI, EsSalud
Descargar PDF con más información sobre la filiación y rol de los autores.
Metodología
Resumen de la metodología:
- Conformación del GEG: La Dirección de Guías de Práctica Clínica, Farmacovigilancia y Tecnovigilancia, del Instituto de Evaluación de Tecnologías en Salud e Investigación (IETSI) del Seguro Social del Perú (EsSalud), conformó un grupo elaborador de la guía (GEG), que incluyó médicos especialistas y metodólogos.
- Planteamiento de preguntas clínicas: En concordancia con los objetivos y alcances de esta GPC, se formularon las preguntas clínicas.
- Búsqueda de la evidencia para cada pregunta: Para cada pregunta clínica, se realizaron búsquedas de revisiones sistemáticas (publicadas como artículos científicos o guías de práctica clínica). De no encontrar revisiones de calidad, se buscaron estudios primarios, cuyo riesgo de sesgo fue evaluado usando herramientas estandarizadas.
- Evaluación de la certeza de la evidencia: Para graduar la certeza de la evidencia, se siguió la metodología Grading of Recommendations Assessment, Development, and Evaluation (GRADE), y se usaron tablas de Summary of Findings (SoF).
- Formulación de las recomendaciones: El GEG revisó la evidencia recolectada para cada una de las preguntas clínicas en reuniones periódicas, en las que formuló las recomendaciones usando la metodología GRADE, otorgándole una fuerza a cada una. Para ello, se tuvo en consideración los beneficios y daños de las opciones, valores y preferencias de los pacientes, aceptabilidad, factibilidad, equidad y uso de recursos. Estos criterios fueron presentados y discutidos, tomando una decisión por consenso o mayoría simple. Asimismo, el GEG emitió puntos de buenas prácticas clínicas (BPC) sin una evaluación formal de la evidencia, y mayormente en base a su experiencia clínica.
- Revisión externa: La presente GPC fue revisada en reuniones con profesionales representantes de otras instituciones, tomadores de decisiones, y expertos externos.
Flujogramas que resumen el contenido de la GPC
vacio
vacio
1. Diagnóstico de lumbalgia
Descargar PDF con el desarrollo de la pregunta.
Recomendación 1:
Se define lumbalgia como dolor o malestar localizado entre el borde inferior de las últimas costillas y el pliegue inferior glúteo, con o sin irradiación a una o ambas extremidades inferiores, sin que ésta deba ser considerada de origen radicular.
Según el tiempo de duración del dolor, la lumbalgia se clasifica en:
- Aguda: dolor de menos de 6 semanas.
- Subaguda: dolor de 6-12
- Crónica: más de 12 semanas con
Recurrente: lumbalgia aguda en paciente que ha tenido episodios previos de dolor lumbar en una localización similar, con períodos libres de síntomas de tres meses. (Recomendación condicional a favor)
Recomendación 2:
Los signos de alarma en la lumbalgia son: edad mayor a 50 años, antecedentes de neoplasia, síndrome consuntivo sin mejoría con tratamientos habituales, dolor en reposo, fiebre, inmunosupresión, traumatismo previo, osteoporosis, toma de corticoides y síndrome de cauda equina. (Recomendación condicional a favor)
Recomendación 3:
No se sugiere la realización de pruebas de laboratorio o imagen (radiografía, tomografía, resonancia) en pacientes con dolor lumbar agudo o subagudo sin signos de alarma. (Recomendación condicional en contra)
2. Tratamiento no farmacológico
Descargar PDF con el desarrollo de la pregunta.
Recomendación 1:
No se sugiere reposo en cama en pacientes con dolor lumbar agudo o subagudo. (Recomendación condicional en contra)
Recomendación 2:
Se sugiere en pacientes con dolor lumbar agudo o subagudo continuar con la actividad física y mantener las actividades de la vida diaria, incluyendo la actividad laboral, tanto como sea posible. (Recomendación condicional a favor)
Recomendación 3:
No se sugiere implementar programas de escuela de espalda para pacientes con lumbalgia aguda y subaguda. (Recomendación condicional en contra)
Recomendación 4:
Recomendamos la terapia manual de manipulación y movilización de tejidos blandos brindada por un médico rehabilitador o terapista físico en un servicio de rehabilitación para el manejo de lumbalgia aguda y subaguda, de acuerdo a disponibilidad del servicio. (Recomendación fuerte a favor)
Recomendación 5:
No se sugiere usar los soportes lumbares (fajas o corsés) para el manejo de lumbalgia aguda y subaguda.(Recomendación condicional en contra)
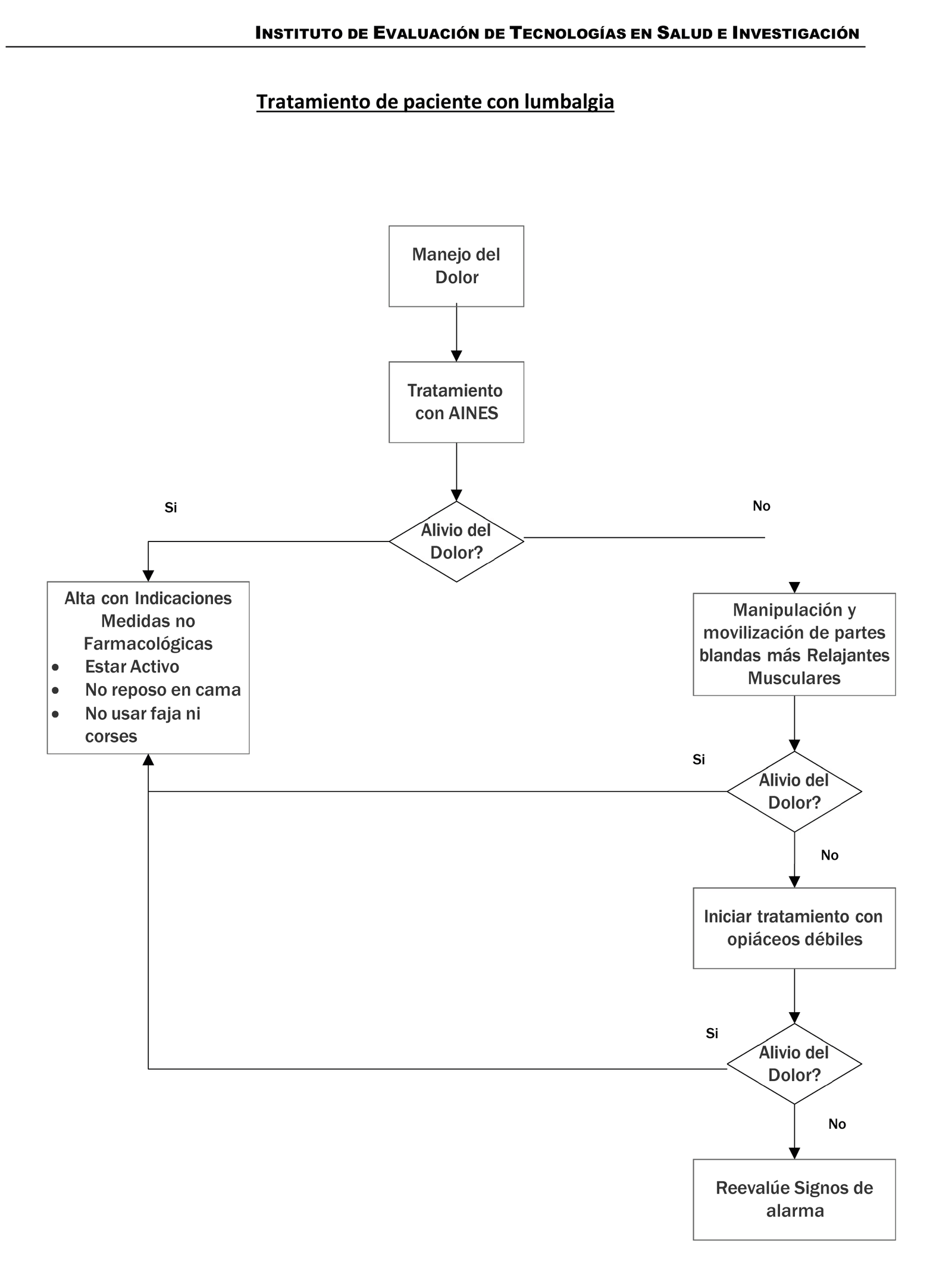
3. Tratamiento farmacológico
Descargar PDF con el desarrollo de la pregunta.
Recomendación 1:
No recomendamos la utilización de paracetamol – independientemente de la dosis – como monoterapia de primera elección en el tratamiento de la lumbalgia aguda y subaguda. (Recomendación fuerte en contra)
Recomendación 2:
Se sugiere AINEs como tratamiento de primera línea de la lumbalgia aguda y subaguda. (Recomendación condicional a favor)
Recomendación 3:
Se sugiere agregar un relajante muscular si el dolor lumbar agudo y subagudo persiste tras iniciar el tratamiento con AINE. (Recomendación condicional a favor)
Recomendación 4:
Se sugiere el uso de un opiáceo débil (tramadol, codeína) si la lumbalgia aguda y subaguda persiste tras iniciar el tratamiento con AINE y relajante muscular. (Recomendación condicional a favor)
Referencias bibliográficas
- Savigny P, Kuntze S, Watson P, Underwood M, Ritchie G , Cotterell M, Hill D, Browne N, Buchanan E, Coffey P, Dixon P, Drummond C, Flanagan M, Greenough,C, Griffiths M, Halliday-Bell J, Hettinga D, Vogel S, Walsh Low Back Pain: early management of persistent non-specific low back pain. London, 2009: National Collaborating Centre for Primary Care and Royal College of General Practitioners.
- Goertz M, Thorson D, Bonsell J, Bonte B, Campbell R, Haake B, Johnson K, Kramer C, Mueller B, Peterson S, Setterlund L, Timming Institute for Clinical Systems Improvement. Adult Acute and Subacute Low Back Pain. Updated November 2012.
- Bundesärztekammer (BÄK), Kassenärztliche Bundesvereinigung (KBV), Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften (AWMF). Nationale VersorgungsLeitlinie Kreuzschmerz – Kurzfassung, 1. Auflage. Version 5. 2010 zuletzt verändert: Oktober Available from: http://www.kreuzschmerz.versorgungsleitlinien.de; [cited: 21.12.2015]; DOI: 10.6101/AZQ/000251
- Pérez Irazusta I., Alcorta Michelena I., Aguirre Lejarcegui G., Aristegi Racero G., Caso Martinez J., Esquisabel Martinez R., López de Goicoechea Fuentes AJ., Mártinez Eguía B., Pérez Rico M., Pinedo Otaola S., Sainz de Rozas Aparicio R. Guía de Práctica Clínica sobre Lumbalgia GPC 2007/1. Vitoria-Gasteiz.
- Ministerio de Salud del Perú. Documento Técnico: Metodología para la Elaboración de Guías de Práctica Clínica. Resolución Ministerial 414-2015-MINSA Julio
- The ADAPTE Collaboration (2009). The ADAPTE Process: Resource toolkit for Guideline Version 2.0. Available from: http://www.g-i-n.net
- Hospital Nacional Dos de Mayo, Ministerio de Guías de Práctica Clínica: Servicio de Medicina Física y Rehabilitación: Lumbalgia. Lima 2010.
- Higgins JPT, Altman DG, Gotzsche PC, Juni P, Oxman AD, Savovic J, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised BMJ 2011;343:d5928.
- Shea BJ, Grimshaw JM, Wells GA, Boers M, Andersson N, Hamel C, et Development of AMSTAR: a measurement tool to assess the methodological quality of systematic reviews. BMC Med Res Methodol. 2007 Feb 15; 7:10.
- Airaksinen O, Brox JI, Cedraschi C, et Chapter 4 European guidelines for the management of chronic nonspecific low back pain. Eur Spine J 2006;15(Suppl. 2):S192– S300.
- Nielens H, Van Zundert J, Mairiaux P, Gailly J, Van Den Hecke N, Mazina D, et al. Chronic low back pain. Good Clinical practice (GCP). Brussels: Belgian Health Care Knowledge Centre (KCE); KCE reports 48 C (D/2006/10.273/71).
- Manchikanti L, Falco FJE, Singh V, et al. An Update of Comprehensive Evidence-Based Guidelines for Interventional Techniques in Chronic Spinal Pain. Part I: Introduction and General Pain Physician 2013;16:S1-S48.
- Manchikanti L, Abdi S, Atluri S, et An Update of Comprehensive Evidence-Based Guidelines for Interventional Techniques in Chronic Spinal Pain. Part II: Guidance and Recommendations. Pain Physician 2013; 16:S49-S283.
- Manejo de rehabilitación del dolor musculo esquelético agudo y crónico: Lumbalgia. Año de publicación no precisado.
- Agence Nationale d-Accreditation et d’Evaluation en Santé. Prise en charge diagnostique et therapeutique des lombalgies et lombosciatiques comunes de moins de trois mois d’evolution. Paris Cedex
- The Norwegian Back Pain Network- The communication Acute low back pain. Interdisciplinary clinical guidelines. Oslo, 2002: The Norwegian Back Pain Network.
- Australian Acute Musculoskeletal Pain Guidelines Evidence-based management of acute musculoskeletal pain. Brisbane, 2003: Australian Academic Press Pty Ltd.
- Bekkering GE, Hendriks HJM, Koes BW, et Dutch Physiotherapy Guidelines for Low Back Pain. Physiotherapy 2003;89:82-95.
- Lopez Roldan VM, Oviedo Mota MA, Guzman Gonzalez JM, et al. Guia clínica para la atención del síndrome doloroso Rev Med IMSS 2003;41(Supl):S123-S130.
- Kendall, N A S, Linton, S J & Main, C J (1997). Guide to Assessing Psycho-social Yellow Flags in Acute Low Back Pain: Risk Factors for Long-Term Disability and Work Loss. Accident Compensation Corporation and the New Zealand Guidelines Group, Wellington, New (Oct, 2004 Edition).
- Chou R, Qaseem A, Snow A, et al. Diagnosis and Treatment of Low Back Pain: A Joint Clinical Practice Guideline from the American College of Physicians and the American Pain Ann Intern Med 2007;147:478-91.
- Chou R, Loeser JD, Owens DK, et Interventional Therapies, Surgery, and Interdisciplinary Rehabilitation for Low Back Pain An Evidence-Based Clinical Practice Guideline From the American Pain Society. Spine 2009;34:1066-77.
- Delitto A, George SZ, van Dillen L, et al. Low Back Pain Clinical Practice Guidelines Linked to the International Classification of Functioning, Disability, and Health from the Orthopaedic Section of the American Physical Therapy Association. J Orthop Sports Phys Ther 2012;42:A1-A57.
- Goertz M, Thorson D, Bonsell J, Bonte B, Campbell R, Haake B, Johnson K, Kramer C, Mueller B, Peterson S, Setterlund L, Timming Institute for Clinical Systems Improvement. Adult Acute and Subacute Low Back Pain. Updated November 2012.
- Guevara-Lopez U, Covarrubias-Gomez A, Elias-Dib J, Reyes-Sanchez A, Rodriguez-Reyna Parámetros de práctica para el manejo de dolor de espalda baja. Cir Cir 2011;79:286- 302.
- Department of Labor and Employment, State of Low back pain Clinical Treatment Guidelines. Colorado, 2014.
- Towards Optimize Practice and Alberta Institute of Health Economics. Guidelines for the Evidence-Informed Primary Care Management of Low Back Alberta, 2011. 2nd Edition.
- Chiodo AM, and the University of Michigan Low Back Pain Guideline Team. Guidelines for Clinical Care Ambulatory: Acute Low Back Michigan, 2010.
- Staal JB, Hendriks EJM, Heijmans M, et al. KNGF-richtlijn Lage rugpijn. Amersfoort, 2013. Koninklijk Nederlands Genootschap voor Fysiotherapie (KNGF).
- Diagnóstico, Tratamiento y Prevención de Lumbalgia Aguda y Crónica en el primer nivel de atención. México: Secretaría de 2009.
- Negrini S, Giovanonni S, Minozzi S, et al. Diagnostic therapeutic flow-charts for low back pain patients: the Italian clinical Eura Medicophys 2006; 42:151-70.
- Jara Leonelli LA, Lopetegui Olivera C, Monnier Berner Protocolo de Referencia- Contrarreferencia Patología de Columna Lumbar Servicio de Salud Araucania Sur. Chile, 2011.
- Petit A, Fassier J-B, Rousseau S, Mairiaux P, Roquelaure French good practice guidelines for medical and occupational surveillance of the low back pain risk among workers exposed to manual handling of loads. Annals of Occupational and Environmental Medicine 2015;27:18.
- Pairoa Amadori Servicio de Salud Aconcagua. Protocolo Lumbalgia. Chile, 2011.
- Marin Plaza Subred Victoria. Protocolo de Referencia y Contrarreferencia de Lumbalgia. Chile, año no especificado.
- Rossignol M, Arsenault B, Dionne C, et al. Clinic on low back pain in interdisciplinary practice (CLIP) guidelines. Montreal, 2007: Direction de Santé Publique, Agence de la Santé et des Services Sociaux de
- Servicio de Salud O’Higgins. Protocolos de Referencia y Contrarreferencia O’Higgins: Chile, 2011.
- Balagué F, Mannion AF, Pellisé F, Cedraschi C. Non-specific low back pain. 2012 Feb 4;379(9814):482-91. doi: 10.1016/S0140-6736(11)60610-7. Epub 2011 Oct 6. Review. PubMed PMID: 21982256.
- Hamilton Acute back pain. Medicine 2008:37(1):17-22)
- Manusov Evaluation and diagnosis of low back pain. Prim Care. 2012 Sep;39(3):471-9. doi: 10.1016/j.pop.2012.06.003. Review. PubMed PMID: 22958556.
- Borenstein D. Mechanical low back pain–a rheumatologist’s view. Nat Rev Rheumatol. 2013 Nov;9(11):643-53. doi: 1038/nrrheum.2013.133. Epub 2013 Sep 10. Review. PubMed PMID: 24018549.
- Henschke N, Maher CG, Refshauge KM. A systematic review identifies five «red flags» to screen for vertebral fracture in patients with low back J Clin Epidemiol. 2008 Feb;61(2):110-118. doi: 10.1016/j.jclinepi.2007.04.013
- Henschke N, Maher CG, Ostelo RWJG, de Vet HCW, Macaskill P, Irwig Red flags to screen for malignancy in patients with low-back pain. Cochrane Database of Systematic Reviews 2013, Issue 2. Art. No.: CD008686. DOI: 10.1002/14651858.CD008686.pub2.
- Williams CM, Henschke N, Maher CG, van Tulder MW, Koes BW, Macaskill P, Irwig L. Red flags to screen for vertebral fracture in patients presenting with low-back pain. Cochrane Database of Systematic Reviews 2013, Issue Art. No.: CD008643. DOI: 10.1002/14651858.CD008643.pub2.
- Raison NT, Alwan W, Abbot A, Farook M, Khaleel A. The reliability of red flags in spinal cord Arch Trauma Res. 2014 Mar 30;3(1):e17850. doi:10.5812/atr.17850.
- van Rijn RM, Wassenaar M, Verhagen AP, Ostelo RW, Ginai AZ, de Boer MR, van Tulder MW, Koes BW. Computed tomography for the diagnosis of lumbar spinal pathology in adult patients with low back pain or sciatica: a diagnostic systematic review. Eur Spine J. 2012 Feb;21(2):228-39. doi:10.1007/s00586-011-2012-2
- Wassenaar M, van Rijn RM, van Tulder MW, Verhagen AP, van der Windt DA, Koes BW, de Boer MR, Ginai AZ, Ostelo RW. Magnetic resonance imaging for diagnosing lumbar spinal pathology in adult patients with low back pain or sciatica: a diagnostic systematic review. Eur Spine J. 2012 Feb;21(2):220-7. doi:10.1007/s00586-011-2019-8.
- Graves JM, Fulton-Kehoe D, Jarvik JG, Franklin GM. Early imaging for acute low back pain: one-year health and disability outcomes among Washington State workers. Spine (Phila Pa 1976). 2012 Aug 15;37(18):1617-27. PubMed PMID:
- Hilal K, Sajjad Z, Sayani R, Khan D. Utility of limited protocol magnetic resonance imaging lumbar spine for nerve root compression in a developing country, is it accurate and cost effective? Asian Spine 2013 Sep;7(3):184-9. doi: 10.4184/asj.2013.7.3.184
- Dahm KT, Brurberg KG, Jamtvedt G, Hagen KB. Advice to rest in bed versus advice to stay active for acute low-back pain and sciatica. Cochrane Database of Systematic Reviews 2010, Issue Art. No.: //CD007612. DOI: 10.1002/14651858.CD007612.pub2.
- Friedman BW, Rothberg S. Complementary Interventions for Emergency Department Patients With Acute or Sub-Acute Mechanical Low Back Annals of Emergency Medicine 2015; 66(4S):S114
- Mc Intosh G, Hall Low back pain (acute). Clinical Evidence 2008;10:1102.
- Verbunt JA, Sieben J, Vlaeyen JW, Portegijs P, André Knottnerus J. A new episode of low back pain: who relies on bed rest? Eur J 2008 May;12(4):508-16.
- Little P, Lewith G, Webley F, Evans M et al. Randomised controlled trial of Alexander technique lessons, exercise, and massage (ATEAM) for chronic and recurrent back pain. 2008; 337 :a884.
- Hayden JA, van Tulder MW, Malmivaara A, Koes BW. Exercise therapy for treatment of non-specific low back pain. Cochrane Database of Systematic Reviews, Issue 3 2006. Chichester: John Wiley & Sons Ltd;
- UK Back pain exercise and manipulation (UKBEAM) Trial United Kingdom back pain exercise and manipulation (UK BEAM) randomised trial: Cost effectiveness of physical treatments for back pain in primary care. BMJ. 2004; 329 (7479):1381-1385.
- Kuukkanen T, Mälkiä E. Effects of a three-month therapeutic exercise programme on flexibility in subjects with low back Physiother Res Int. 2000; 5 (1):46-61.
- Maul I, Läubli T, Oliveri M, Krueger H. Long-term effects of supervised physical training in secondary prevention of low back Eur Spine J. 2005; 14 (6):599-611.
- Mannion AF, Müntener M, Taimela S, Dvorak J. Comparison of three active therapies for chronic low back pain: results of a randomized clinical trial with one-year follow-up. 2001; 40 (7):772-778.
- Schaafsma F, Schonstein E, Whelan KM, et Physical conditioning programs for improving work outcomes in workers with back pain (review). Cochrane Database Syst Rev 2010:CD001822.
- Kool J, Bachmann S, Oesch P, et al. Function-centered rehabilitation increases work days in patients with nonacute nonspecific low back pain: 1-year results from a randomized controlled Arch Phys Med Rehabil 2007;88:1089-94.
- Wright A, Lloyd-Davies A, Williams S, et al. Individual active treatment combined with group exercise for acute and subacute low back Spine 2005;30:1235-41.
- Hagen KB, Hilde G, Jamtvedt G, Winnem M. Bed rest for acute low-back pain and sciatica. Cochrane Database Syst Rev 2004;(4):CD001254.
- Hilde G, Hagen KB, Jamtvedt G, Winnem Advice to stay active as a single treatment for low-back pain and sciatica [Systematic Review]. Cochrane Database of Systematic Reviews 2006;(1).
- Oesch P, Kool J, Hagen KB, Bachmann S. Effectiveness of exercise on work disability in patients with non-acute non-specific low back pain: Systematic review and meta-analysis of randomised controlled J Rehabil Med. 2010 Mar;42(3):193-205. doi: 10.2340/16501977-0524
- Van der Giessen RN, Speksnijder CM, Helders PJ. The effectiveness of graded activity in patients with non-specific low-back pain: a systematic review. Disabil Rehabil. 2012; 34(13):1070-6. doi: 3109/09638288.2011.631682.
- Hidalgo B, Detrembleur C, Hall T, Mahaudens P, Nielens The efficacy of manual therapy and exercise for different stages of non-specific low back pain: an update of systematic reviews. J Man Manip Ther. 2014 May;22(2):59-74. doi: 10.1179/2042618613Y.0000000041
- Yamato TP, Maher CG, Saragiotto BT, Hancock MJ, Ostelo RWJG, Cabral CMN, Menezes Costa LC, Costa LOP. Pilates for low back pain. Cochrane Database of Systematic Reviews 2015, Issue Art. No.: CD010265. DOI: 10.1002/14651858.CD010265.pub2.
- Aluko A, DeSouza L, Peacock J. The effect of core stability exercises on variations in acceleration of trunk movement, pain, and disability during an episode of acute nonspecific low back pain: a pilot clinical J Manipulative Physiol Ther. 2013 Oct;36(8):497-504.e1-3. doi: 10.1016/j.jmpt.2012.12.012
- Hagen EM, Ødelien KH, Lie SA, Eriksen HR. Adding a physical exercise programme to brief intervention for low back pain patients did not increase return to work. Scand J Public 2010 Nov;38(7):731-8. doi: 10.1177/1403494810382472
- Fritz JM, Magel JS, McFadden M, Asche C, Thackeray A, Meier W, Brennan Early Physical Therapy vs Usual Care in Patients With Recent-Onset Low Back Pain: A Randomized Clinical Trial. JAMA. 2015 Oct 13;314(14):1459-67. doi: 10.1001/jama.2015.11648.
- Heymans MW, van Tulder MW, Esmail R, Bombarider C, Koes Escuela de espalda para el dolor lumbar inespecífico. (Revisión Cochrane traducida). En: La Biblioteca Cochrane Plus, 2005 Número 2 Oxford: Update Software Ltd Disponible en: http://update.software.com. (Traducida de The Cochrane Library, 2005 Issue 2 Chichester, UK: John Wiley ¬Sons, Ltd 2006.
- Poquet N, Lin CWC, Heymans MW, van Tulder MW, Esmail R, Koes BW, Maher CG. Back schools for acute and subacute non-specific low-back Cochrane Database of Systematic Reviews 2016, Issue 4. Art. No.: CD008325. DOI: 10.1002/14651858.CD008325.pub2.
- Tutzschke R, Anders C, Borys C, Nodop S, Rößler O, Strauß B, Scholle [Evaluation of the German new back school: muscular physiological characteristics]. Schmerz. 2014 Apr;28(2):166-74. doi: 10.1007/s00482-014-1390-x. German.
- Calmels P, Queneau P, Hamonet C, Le Pen C, Maurel F, Lerouvreur C, Thoumie Effectiveness of a lumbar belt in subacute low back pain: an open, multicentric, and randomized clinical study. Spine (Phila Pa 1976). 2009 Feb 1;34(3):215-20.doi: 10.1097/BRS.0b013e31819577dc.
- Davies RA, Maher CG, Hancock MJ. A systematic review of paracetamol for non-specific low back Eur Spine J. 2008 Nov; 17(11):1423-30. doi:10.1007/s00586-008-0783-x.
- Lasko B, Levitt RJ, Rainsford KD, Bouchard S, Rozova A, Robertson S. Extended-release tramadol/paracetamol in moderate-to-severe pain: a randomized, placebo-controlled study in patients with acute low back pain. Curr Med Res Opin. 2012 May; 28(5):847-57. doi: 10.1185/03007995.2012.681035. Epub 2012 Apr 25. PubMed PMID: 22458917.
- Roelofs PDDM, Deyo RA, Koes BW, Scholten RJPM, van Tulder MW. Non-steroidal anti- inflammatory drugs for low back pain. Cochrane Database of Systematic Reviews 2008, Issue 1. No.: CD000396. DOI: 10.1002/14651858.CD000396.pub3.
- Abdel Shaheed C, Maher CG, Williams KA, McLachlan AJ. Interventions available over the counter and advice for acute low back pain: systematic review and meta-analysis. J Pain. 2014 Jan;15(1):2-15. doi: 1016/j.jpain.2013.09.016
- Moore RA, Barden J. Systematic review of dexketoprofen in acute and chronic pain. BMC Clin Pharmacol. 2008 Oct 31;8:11. doi: 10.1186/1472-6904-8-11. Review. PubMed PMID: 18976451; PubMed Central PMCID:
- Van Tulder MW, Touray T, Furlan AD, Solway S, Bouter Muscle relaxants for nonspecific low back pain. Cochrane Database Syst Rev 2003;(2):CD004252.
- Berry H, Hutchinson DR. Tizanidine and ibuprofen in acute low-back pain: results of a double-blind multicentre study in general J Int Med Res 1988; 16(2):83-91.
- Borenstein DG, Lacks S, Wiesel Cyclobenzaprine and naproxen versus naproxen alone in the treatment of acute low back pain and muscle spasm. Clin Ther 1990; 12(2):125-131.
- Machado LA, Kamper SJ, Herbert RD, Maher CG, McAuley JH. Analgesic effects of treatments for non-specific low back pain: a meta-analysis of placebo-controlled randomized Rheumatology (Oxford). 2009 May;48(5):520- 7.doi:10.1093/rheumatology/ken470.
- Cabitza P, Randelli Efficacy and safety of eperisone in patients with low back pain: a double blind randomized study. Eur Rev Med Pharmacol Sci. 2008 Jul-Aug; 12(4):229-35.
- Chandanwale AS, Chopra A, Goregaonkar A, Medhi B, Shah V, Gaikwad S, Langade DG, Maroli S, Mehta SC, Naikwadi A, Pawar DR. Evaluation of eperisone hydrochloride in the treatment of acute musculoskeletal spasm associated with low back pain: a randomized, double-blind, placebo-controlled trial. J Postgrad Med. 2011 Oct-Dec; 57(4):278-85. doi: 4103/0022-3859.90076.
- Rao R, Panghate A, Chandanwale A, Sardar I, Ghosh M, Roy M, Banerjee B, Goswami A, Kotwal Clinical comparative study: efficacy and tolerability of tolperisone and thiocolchicoside in acute low back pain and spinal muscle spasticity. Asian Spine J. 2012 Jun;6(2):115-22. doi: 10.4184/asj.2012.6.2.115.
- Kumar S, Rani S, Siwach R, Verma P. To compare the efficacy and safety of fixed dose combination of thiocolchicoside and aceclofenac versus chlorzoxazone, aceclofenac and paracetamol in patients with acute lower backache associated with muscle spasm. Int J Appl Basic Med Res. 2014 Jul;4(2):101-5. doi:10.4103/2229-516X.136789.
- Malanga GA, Ruoff GE, Weil AJ, Altman CA, Xie F, Borenstein DG. Cyclobenzaprine ER for muscle spasm associated with low back and neck pain: two randomized, double-blind, placebo-controlled studies of identical Curr Med Res Opin. 2009 May; 25(5):1179- 96. doi: 10.1185/03007990902851753.
- Weil AJ, Ruoff GE, Nalamachu S, Altman CA, Xie F, Taylor DR. Efficacy and tolerability of cyclobenzaprine extended release for acute muscle spasm: a pooled analysis. Postgrad 2010 Jul; 122(4):158-69. doi: 10.3810/pgm.2010.07.2182.
- Friedman BW, Dym AA, Davitt M, Holden L, Solorzano C, Esses D, Bijur PE, Gallagher EJ. Naproxen With Cyclobenzaprine, Oxycodone/Acetaminophen, or Placebo for Treating Acute Low Back Pain: A Randomized Clinical Trial. JAMA. 2015 Oct 20;314(15):1572-80. doi: 10.1001/jama.2015.13043
- Katz N, Rauck R, Ahdieh H, Ma T et al. A 12-week, randomized, placebo-controlled trial assessing the safety and efficacy of oxymorphone extended release for opioid-naive patients with chronic low back Curr Med Res Opin. 2007; 23 (1):117-128.
- Schnitzer TJ, Ferraro A, Hunsche E, Kong SX. A comprehensive review of clinical trials on the efficacy and safety of drugs for the treatment of low back pain. J Pain Symptom Manage 2004; 28(1):72-95.
- Palangio M, Morris E, Doyle RT, , Dornseif BE, Valente TJ. Combination hydrocodone and ibuprofen versus combination oxycodone and acetaminophen in the treatment of moderate or severe acute low back pain. Clin Ther 2002; 24(1):87-99.
- Andrews JC, Schünemann HJ, Oxman AD, Pottie K, Meerpohl JJ, Coello PA, et al. GRADE guidelines: Going from evidence to recommendation-determinants of a recommendation’s direction and strength. J Clin Epidemiol 2013; 66: 726-35.
- Andrews J, Guyatt G, Oxman AD, Alderson P, Dahm P, Falck-Ytter Y, et GRADE guidelines: 14. Going from evidence to recommendations: the significance and presentation of recommendations. J Clin Epidemiol 2013; 66: 719-25.
Si tienes comentarios sobre el contenido de las guías de práctica clínica, puedes comunicarte con IETSI-EsSalud enviando un correo a ietsi.gpc@gmail.com

SUGERENCIAS
Si has encontrado un error en esta página web o tienes alguna sugerencia para su mejora, puedes comunicarte con EviSalud enviando un correo a evisalud@gmail.com